The journey of family planning is deeply personal, marked by hopes, dreams, and often, significant decisions. For couples who have decided their family is complete, permanent contraception offers a profound sense of closure and liberation. The two primary options available are tubal ligation for women and vasectomy for men. While both are highly effective, the prevailing narrative often overlooks a critical distinction: vasectomy, in a vast majority of cases, presents a significantly safer, less invasive, and more straightforward pathway to permanent fertility control. This is a story that deserves to be told, understood, and embraced by those navigating this crucial life choice.
For generations, the onus of contraception, temporary or permanent, has largely fallen upon women. From daily pills to intricate IUDs, and finally to the surgical permanence of tubal ligation, it is often the female partner who bears the physical, emotional, and sometimes, financial burden. This historical imbalance has, perhaps inadvertently, overshadowed the remarkable safety and efficacy of vasectomy, relegating it to a secondary, often misunderstood, option. Yet, when we strip away societal norms and delve into the medical realities of each procedure, a compelling case emerges for vasectomy as the safer choice, offering a smoother journey and fewer potential pitfalls.
To truly appreciate this difference, we must embark on a detailed exploration of both procedures, examining their intricacies, the experience of the patient, and the spectrum of potential risks and benefits. Only then can we illuminate the often-unacknowledged advantages of vasectomy, empowering couples with knowledge that transcends outdated perceptions and prioritizes genuine well-being.
The Female Path: Understanding Tubal Ligation – A Journey into the Abdomen
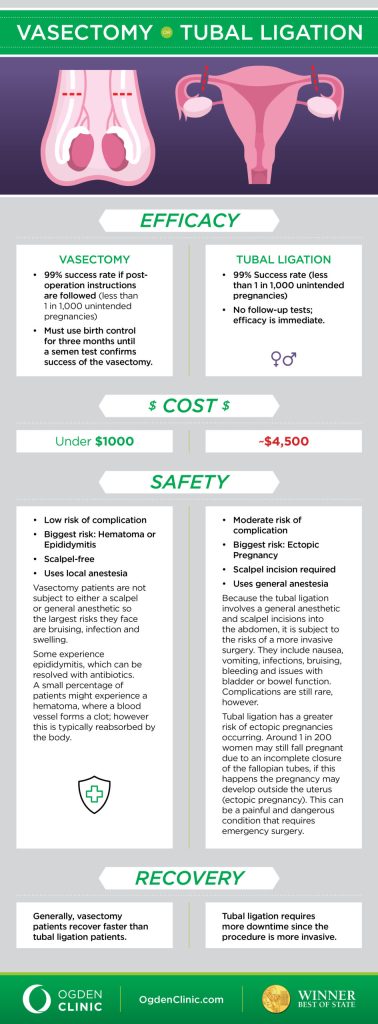
Tubal ligation, often colloquially referred to as "getting one’s tubes tied," is a permanent birth control method for women that involves blocking or severing the fallopian tubes, preventing eggs from reaching the uterus and sperm from reaching the eggs. While undoubtedly effective, the procedure inherently carries a greater degree of invasiveness and, consequently, a higher risk profile than vasectomy.
The Surgical Landscape: Navigating the Abdominal Cavity
The most common approach for tubal ligation is laparoscopy, a minimally invasive surgical procedure that still requires entering the abdominal cavity. Imagine the scenario: the patient is prepped for surgery, a moment often filled with a potent mix of anticipation and apprehension. The very first step, administering general anesthesia, immediately introduces a layer of risk absent in most vasectomies. General anesthesia, while incredibly safe in modern medicine, is not without its own set of potential complications. These can range from minor issues like nausea, vomiting, and a sore throat, to more serious concerns such as adverse drug reactions, respiratory complications (e.g., aspiration pneumonia, laryngospasm), cardiovascular events (e.g., arrhythmias, hypotension), and even, in extremely rare cases, anaphylaxis or death. For a procedure that is elective and primarily for contraception, these systemic risks, however small, are a significant consideration.
Once under general anesthesia, the surgeon makes one or more small incisions, typically near the navel and possibly lower in the abdomen. A specialized instrument called a trocar is inserted through the incision, and the abdominal cavity is then inflated with carbon dioxide gas. This process, known as insufflation, creates space for the surgeon to visualize the pelvic organs and work with instruments. While essential for the procedure, insufflation itself can cause discomfort (e.g., shoulder pain from diaphragmatic irritation) and carries risks such as gas embolism or injury to internal organs during trocar insertion.
Through these small incisions, a laparoscope (a thin, lighted tube with a camera) is inserted, allowing the surgeon to view the fallopian tubes on a monitor. Other instruments are then introduced to block or sever the tubes. There are several methods for achieving tubal occlusion:
- Cutting and Tying: A segment of the fallopian tube is removed, and the remaining ends are tied off.
- Cauterization (Electrocautery): The tubes are burned and sealed using an electrical current.
- Clips or Rings: Small plastic or titanium clips or rings are placed on the fallopian tubes to block them.
Each method has its own nuances and potential for complications, such as incomplete occlusion, which can lead to rare but devastating ectopic pregnancies (where the fertilized egg implants outside the uterus, often in the fallopian tube itself).
Less commonly, tubal ligation may be performed via minilaparotomy, which involves a slightly larger abdominal incision (usually 2-3 inches) but does not require a laparoscope. This approach is sometimes preferred immediately after childbirth (postpartum tubal ligation) when the uterus is still enlarged and the fallopian tubes are more accessible. While avoiding some of the risks of laparoscopy, it entails a larger incision and potentially a longer recovery. Historically, hysteroscopic methods (like Essure) were also available, involving coils inserted through the cervix, but these have largely been discontinued due to safety concerns and patient dissatisfaction.
The Post-Operative Landscape: Recovery and Potential Complications
Following tubal ligation, the recovery period is typically more involved and longer than that for a vasectomy. Patients can expect:
- Pain: Moderate to severe abdominal pain is common, often requiring prescription pain medication. The pain can stem from the incisions, the internal manipulation of organs, and residual gas from insufflation. Shoulder pain is a common complaint due to diaphragmatic irritation from the CO2 gas.
- Activity Restriction: Women are usually advised to avoid strenuous activity, heavy lifting, and sexual intercourse for several weeks to allow for proper healing and to prevent complications.
- Hospital Stay: While often performed as an outpatient procedure, some women may require an overnight stay, especially if there are complications or if it’s performed in conjunction with other procedures (like a C-section).
The spectrum of potential complications associated with tubal ligation, though generally rare, is broader and often more serious due to the nature of intra-abdominal surgery:
- Infection: At the incision sites or, more seriously, internal pelvic infection.
- Bleeding: Hematoma formation at the incision sites or internal hemorrhage, which can require further intervention.
- Damage to Adjacent Organs: During trocar insertion or instrument manipulation, there is a risk of inadvertently perforating or injuring the bowel, bladder, or major blood vessels. While rare, these complications can be life-threatening and necessitate immediate, more extensive corrective surgery.
- Adhesions: Scar tissue can form internally, potentially leading to chronic pelvic pain or, in severe cases, bowel obstruction years after the procedure.

