The first cry. The skin-to-skin embrace. The overwhelming rush of love and instinct. For many new mothers, the vision of breastfeeding is an integral part of this cherished early narrative – a serene, natural communion between mother and child, a seamless dance of instinct and nourishment. We envision a baby rooting instinctively, latching deeply, feeding contentedly, and growing robustly. We read the books, attend the classes, and absorb the wisdom, preparing ourselves for what seems like the most natural act in the world.
But sometimes, reality paints a different picture. The soft sighs of contentment are replaced by frustrated cries, frantic head-bobbing, and a mother’s escalating sense of inadequacy. The deep, satisfying suckle gives way to shallow, painful nibbles that leave nipples sore and spirits frayed. The dream of effortless bonding can quickly transform into a battle of wills, a perplexing puzzle of ineffective attempts, and a gnawing doubt about one’s own maternal capabilities. This is the often-unspoken truth for countless new moms: the journey to comfortable and effective breastfeeding can be fraught with unexpected challenges, chief among them nipple confusion and latch issues.
This guide is for the knowledgeable mom – the one who has done her research, who understands the profound benefits of breastfeeding, and who is determined to navigate these early waters with informed resilience. It’s a comprehensive journey into the physiological intricacies of breastfeeding, the subtle yet significant distinctions between breast and artificial nipples, and the multifaceted reasons behind latch difficulties. More than just a list of problems, this is a roadmap to understanding, preventing, and ultimately overcoming these hurdles, empowering you with the insights and strategies needed to reclaim the comfort and joy of your breastfeeding experience. We’ll tell a story not just of struggle, but of informed perseverance, leading to the profound satisfaction of a deep, comfortable latch for both you and your baby.
The Instinctual Symphony: Understanding the Breastfeeding Blueprint
Before we delve into the complexities of challenges, it’s crucial to understand the exquisite biological ballet that should unfold. Breastfeeding is a finely tuned symphony of innate reflexes and physiological responses, honed over millennia of human evolution. When this symphony plays without interruption, it is a marvel.
The Newborn’s Innate Toolkit: From the moment of birth, a healthy newborn arrives equipped with a remarkable set of reflexes designed specifically for feeding.
- Rooting Reflex: A gentle touch to the cheek or mouth triggers the baby to turn their head towards the stimulus, mouth open, searching for the nipple. This is their primal "find the food" mechanism.
- Suck Reflex: Once the nipple is in the mouth, rhythmic suckling begins, a complex coordination of jaw, tongue, and swallowing.
- Gag Reflex: Positioned further back in the mouth, this protects against aspiration, but also plays a role in how deeply a baby can take the breast.
- Swallowing Reflex: Coordinated with sucking, this ensures milk moves from mouth to stomach.
These reflexes are strongest in the first hour or two after birth, often referred to as the "golden hour." Skin-to-skin contact during this time is not just for bonding; it’s a powerful biological imperative that helps initiate breastfeeding. The familiar scent of the mother, the warmth, the sound of her heartbeat – all create an optimal environment for the baby to self-attach, often performing the "breast crawl" to find the nipple independently. This initial, unassisted latch is frequently the deepest and most instinctive, laying a foundational neural pathway for future feeds.
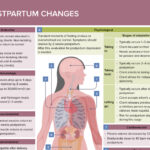
The Mother’s Physiological Response: Concurrently, the mother’s body is primed. The act of suckling, even rooting, triggers the release of oxytocin, the "love hormone," which is responsible for the milk ejection reflex (MER), or "let-down." This reflex contracts the tiny muscle cells around the milk-producing alveoli, pushing milk through the ducts towards the nipple. Prolactin, the "milk-making hormone," signals the breasts to produce more milk based on demand. The breast itself is a dynamic organ, its nipple and areola capable of changing shape and texture in response to stimulation, becoming erect and pliable, ready for the baby’s wide gape.
The ideal breastfeeding scenario is one where the baby’s instincts align perfectly with the mother’s physiology: a wide-mouthed baby takes a deep, asymmetrical latch, drawing in not just the nipple but a significant portion of the areola. The tongue cups the breast, creating a vacuum and compressing the milk ducts against the hard palate, efficiently extracting milk. The mother feels a gentle tug, not pain, and hears rhythmic swallowing. This is the blueprint – a natural, comfortable, and highly efficient system. When disruptions occur, it’s often because one or more elements of this intricate design are misaligned or misinterpreted.
Decoding Nipple Confusion: More Than Just a "Preference"
The term "nipple confusion" has been a subject of debate among lactation professionals, with some preferring "latch disruption" or "flow preference." Regardless of the terminology, the phenomenon is real and profoundly challenging for new moms. At its core, nipple confusion describes an infant’s struggle to effectively latch onto the mother’s breast after being introduced to artificial nipples (bottles, pacifiers). It’s not a conscious choice by the baby; rather, it’s a physiological and behavioral adaptation to differing feeding mechanisms that makes switching between them difficult.
What Exactly Is It?
Imagine learning to drive one type of car, say, a stick shift, and then being immediately expected to drive an automatic without any instruction. The muscle memory, the coordination, the expectations of how the vehicle responds – all are different. For a newborn, the breast and a bottle nipple are two fundamentally different "vehicles" for obtaining milk, requiring distinct oral motor skills. When a baby consistently practices the "bottle technique," their oral muscles and neural pathways become accustomed to that specific action, making the "breast technique" feel unfamiliar or even impossible.
The Physiological Discrepancies:
The core of nipple confusion lies in the stark differences between how a baby extracts milk from a breast versus an artificial nipple.
-
Shape and Texture:
- Breast Nipple: Pliable, soft, and changes shape within the baby’s mouth, molding to the contours of their palate and tongue. It’s designed to be stretched and compressed. The areola also plays a crucial role, providing a wide, soft base for the baby to latch onto, not just the nipple tip.
- Bottle Nipple: Typically firmer, more rigid, and maintains a consistent shape. While some brands attempt to mimic breast shape, none can replicate the dynamic nature of a living breast. The texture can also be vastly different, often silicone, which feels distinct from skin.