In the grand tapestry of a woman’s life, threads of ambition, connection, self-discovery, and purpose are interwoven with the fundamental decisions she makes about her body and her future. Among these, the choice regarding reproductive autonomy stands as one of the most significant, shaping not just her immediate path but the entire trajectory of her existence. For many, the journey through various temporary contraceptive methods – with their daily demands, side effects, and anxieties – eventually leads to a profound realization: the desire for an uninterrupted life, one where reproductive decisions are definitive, liberating, and seamlessly integrated into their personal narrative. It is in this pursuit of unwavering control and enduring peace of mind that tubectomy emerges not merely as a medical procedure, but as a cornerstone of convenience and a testament to radical self-empowerment.
This article delves deep into the multifaceted benefits of choosing tubectomy, exploring how this permanent method of contraception can transform a woman’s life from one punctuated by the continuous mental load of family planning into one of seamless flow and boundless opportunity. We aim to tell a story – the story of liberation from the invisible chains of daily reproductive anxiety, the story of reclaiming mental bandwidth, and the story of living a life truly authored by oneself. For the knowledgeable audience, we will navigate the nuances of this choice, appreciating its medical efficacy while celebrating its profound human impact.
The Invisible Burden: Life Before the Uninterrupted Choice
Before we can fully appreciate the liberation offered by tubectomy, it’s crucial to acknowledge the landscape from which many women seek an exit: the often-underestimated mental and physical burden of temporary contraception. For years, decades even, a woman committed to preventing pregnancy navigates a complex world of pills, patches, injections, rings, and IUDs. Each method, while offering varying degrees of effectiveness and convenience, comes with its own set of demands and anxieties that subtly, yet cumulatively, interrupt the rhythm of her life.
Consider the daily pill: a meticulous ritual, tethering her to a specific time, an ever-present thought in the back of her mind. A forgotten pill triggers a cascade of worry, requiring emergency measures, and potentially disrupting work, travel, or social engagements. Beyond the schedule, there’s the ongoing concern about side effects – hormonal fluctuations manifesting as mood swings, weight changes, skin issues, or decreased libido. These aren’t minor inconveniences; they are physiological and psychological intrusions that can impact relationships, career performance, and overall well-being.
Longer-acting reversible contraceptives (LARCs) like IUDs and implants offer a reprieve from daily diligence but introduce their own considerations. While highly effective, they often involve initial discomfort during insertion, potential for irregular bleeding, and the eventual need for removal and replacement. The decision to use a LARC is a significant one, requiring medical appointments, costs, and the acceptance of a foreign object within one’s body for an extended period.
This continuous engagement with contraception creates what can be termed "contraceptive fatigue" – a weariness born from the perpetual need to manage, monitor, and mitigate the risks associated with temporary methods. It’s a subtle but constant hum beneath the surface of daily life, drawing mental energy, financial resources, and emotional bandwidth away from other pursuits. For a woman who has definitively completed her family, or who has made the conscious choice not to have children, this ongoing burden can feel not just inconvenient, but fundamentally misaligned with her life’s trajectory. She seeks not just a method, but a resolution; not just control, but freedom.
Tubectomy: The Medical Resolution
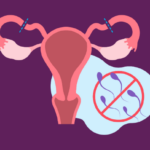
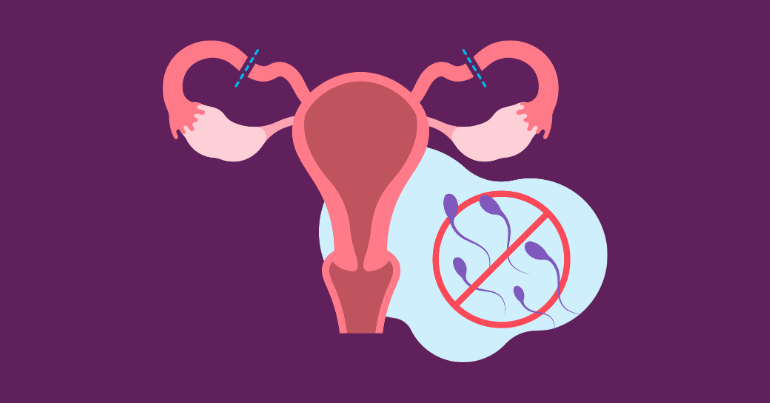
Tubectomy, or female sterilization, is a permanent birth control method that involves blocking or severing the fallopian tubes, thereby preventing eggs from reaching the uterus and sperm from reaching the eggs. It is a highly effective procedure, with a failure rate of less than 1%, making it one of the most reliable forms of contraception available. For a knowledgeable audience, it’s important to understand the various approaches and what the procedure entails, dispelling common misconceptions.
Understanding the Procedure:
The most common surgical approaches for tubectomy include:
-
Laparoscopic Tubal Ligation: This is the most frequently performed method. It is a minimally invasive procedure where a small incision (typically 0.5 to 1.5 cm) is made near the navel. A laparoscope (a thin, lighted tube with a camera) is inserted, allowing the surgeon to view the pelvic organs. One or two additional small incisions may be made in the lower abdomen to insert instruments used to block or cut the fallopian tubes. This can be done using various techniques:
- Ligation: Tying the tubes with sutures.
- Occlusion: Applying rings or clips (like Filshie clips or Hulka clips) to pinch the tubes shut.
- Coagulation: Using electrical current to burn and seal a section of the tubes.
- Excision: Removing a small segment of the tube.
Laparoscopic procedures are often performed on an outpatient basis under general anesthesia, allowing for quicker recovery and less scarring.
-
Mini-Laparotomy: This involves a slightly larger incision (about 2-5 cm) in the lower abdomen, typically just above the pubic hairline. This method is often preferred shortly after childbirth (postpartum tubal ligation) because the uterus is still enlarged and closer to the abdominal wall, making the fallopian tubes more accessible through a smaller incision. It can also be performed as an "interval" procedure (at any time unrelated to pregnancy) if laparoscopy is contraindicated or not available.
-
Hysteroscopic Sterilization (e.g., Essure, now largely discontinued): While historically an option, it’s important to note that devices like Essure, which involved placing coils into the fallopian tubes via the cervix and uterus, have largely been discontinued due to safety concerns and patient complaints. The focus of tubectomy today primarily remains on surgical ligation or occlusion.